


Understanding Male Despair and Solutions
Understanding Male Despair and Solutions


When an acquaintance of mine recently shared his experience with family therapy, I was not shocked to learn that he felt removed from the process—that the therapist created an environment that made him feel isolated and alone. At one point, the therapist raised his voice at the husband and father of two as the husband expressed his frustration in a way that was not combative. I even asked: “Do you think you came across as threatening in any way or combative?” He said, “no.” In fact, he admitted that he was expressing his frustrations clearly and calmly—that he actually felt prepared to share and that the therapist would be open to his feelings, thoughts, and observations.
The more I listened, the more it seemed as though the therapist approached the husband in a way that embraced masculine social norm theory, a theory that essentially sees males (boys and men) as somewhat defective from the get-go because of their reliance on “social norms” that—as some therapists believe—are the reasons males are unable to access their emotions and engage in healthy therapy. By social norms, I’m referring to things like stoicism, toughness, bravado, recklessness, insensitivity, the need for males to recognize themselves as oppressors in order to become healthy. It is these types of misunderstandings of male psychology that lead to sayings like “boys and men commit suicide because they don’t cry enough” or “males are violent because of testosterone” or “males are aggressive because they have grown up thinking they are entitled to things.” A new trend in therapy is relying on oppressor narratives as a way to shame people, particularly men, in therapy. Lisa Selin Davis wrote an interesting piece about “How Therapists Became Social Justice Warriors” in the Free Press back in 2023 that essentially addresses this topic.
These types of observations—not only misunderstand male psychology—but create a litany of distractions that avoid the nature of male psychology that differs from the nature of female psychology, especially when it comes to addressing depression, despair, and attempts at healthy meetings with therapists. Understanding male despair and the male brain is one of our most important endeavors we can undertake at a time when those who do seek treatment are feeling rejected. Numerous studies have shown that males are far more likely to drop out of therapy than females. One such study (Men’s Dropout From Mental Health Services: Results From a Survey of Australian Men Across the Life Span) reveals the depths of this challenge.
“Participants reporting a sense of emasculation (i.e., that presenting to therapy made them feel like “less of a man”) while in therapy experienced higher rates of dropout due to a lack of connection with their therapist. This novel finding underscores the importance of therapists’ capacity to enact “gender competency” when working with men. Gender competency is a novel construct reflecting the capacity to effectively implement male-specific adaptations to therapy, alongside accommodating men’s unique experiences of mental ill health as a potential extension of their experience of masculinity….”
“The overall dropout rate from therapy was 44.8% (n = 855), of which 26.6% (n = 120) accessed therapy once and did not return. The most common reasons for dropout were lack of connection with the therapist (54.9%) and the sense that therapy lacked progress (20.2%).”
This sounds very much like the experience of my acquaintance who eventually dropped out of therapy while his family continued, but I encouraged him to look for another therapist who understands male psychology from a nature lens. The phrase I like to use is the one from Michael Gurian, a therapist who “nurtures the nature.” In this approach, male brain and female brain differences are the guiding principles and the therapy is conducted accordingly.
While the study above uses the phrase “gender competency” to express the difference between males and females, I would encourage a more sex-based term instead because today’s use of sex and gender is often muddied, and the terms are used interchangeably when we know sex is not gender and gender is not sex. How much different would the observation above look and how might men respond if we replaced the words “gender competency” with brain-sex competency or brain-sex difference, focusing more on male and less on masculine. Let’s try it out:
This novel finding underscores the importance of therapists’ capacity to enact
“gender competency”brain-sex competences when working with men.Gender competencyBrain-sex difference is anovelknown construct reflecting the capacity to effectively implement male-specific adaptations to therapy, alongside accommodating men’s unique experiences of mental ill health as a potential extension of their experience at time when there is a greater emphasis on masculinity and an underemphasis on the male brain as distinct from the female brain.of masculinity.”
This isn’t perfect, but it keeps us from distracting ourselves with the masculine social norm theories and the socially constructed gender paradigms that take us away from the first principle, male. The bold phrase I added at the end might be a bit more strident perhaps for a paper like the one above but certainly within bounds when it comes to ensuring the distinctions between male (innate) and masculine (socially constructed). In the study above of just over 1,900 Australian males, the word brain is not mentioned once but the word masculine or masculinity is mentioned 42 times. And it is not as though we should ignore the social barriers that may prevent men from coming forward, but we might actually encourage men to come forward if we explain the logos of male depression and the way it presents in boys and men differently than girls and women and how the different processes in the male brain explain a boy or man’s reactions to all sorts of triggers, traumas, and every day things. In other words, we are telling men that they are different and because they are different (not defective) they can begin to see their uniqueness, with all its splendor and its challenges.
Preparing to Discuss Despair
The story above about my acquaintance came to mind as I was preparing for a symposium in California this week and was reviewing updated data on deaths of despair. I was not surprised to see the disparity between males and females, but I was surprised to see that alcohol related deaths in CA were higher than suicide deaths, a trend that is noticeably different from national data, where suicide deaths and alcohol related deaths happen more or less to the same degree.
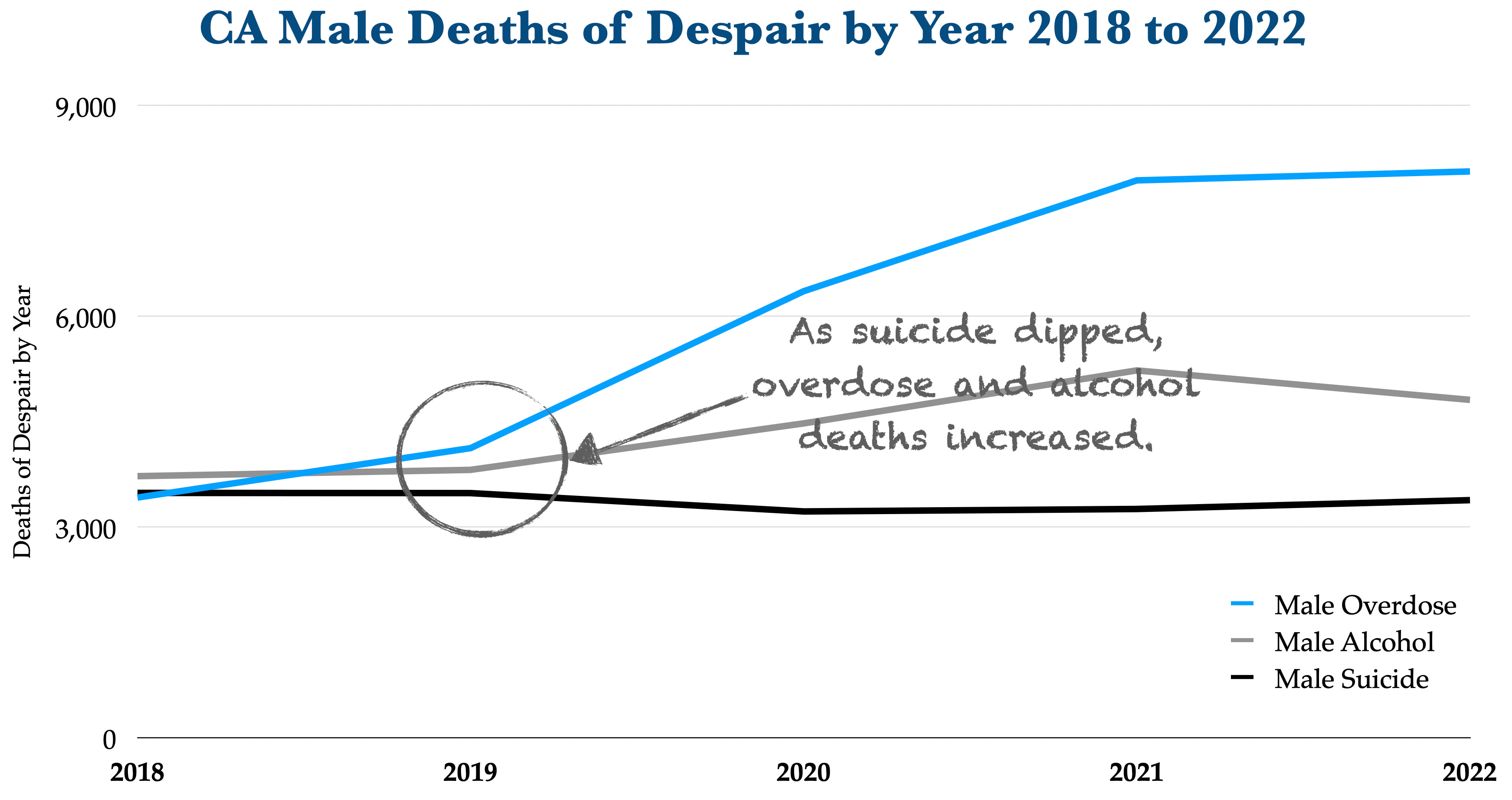
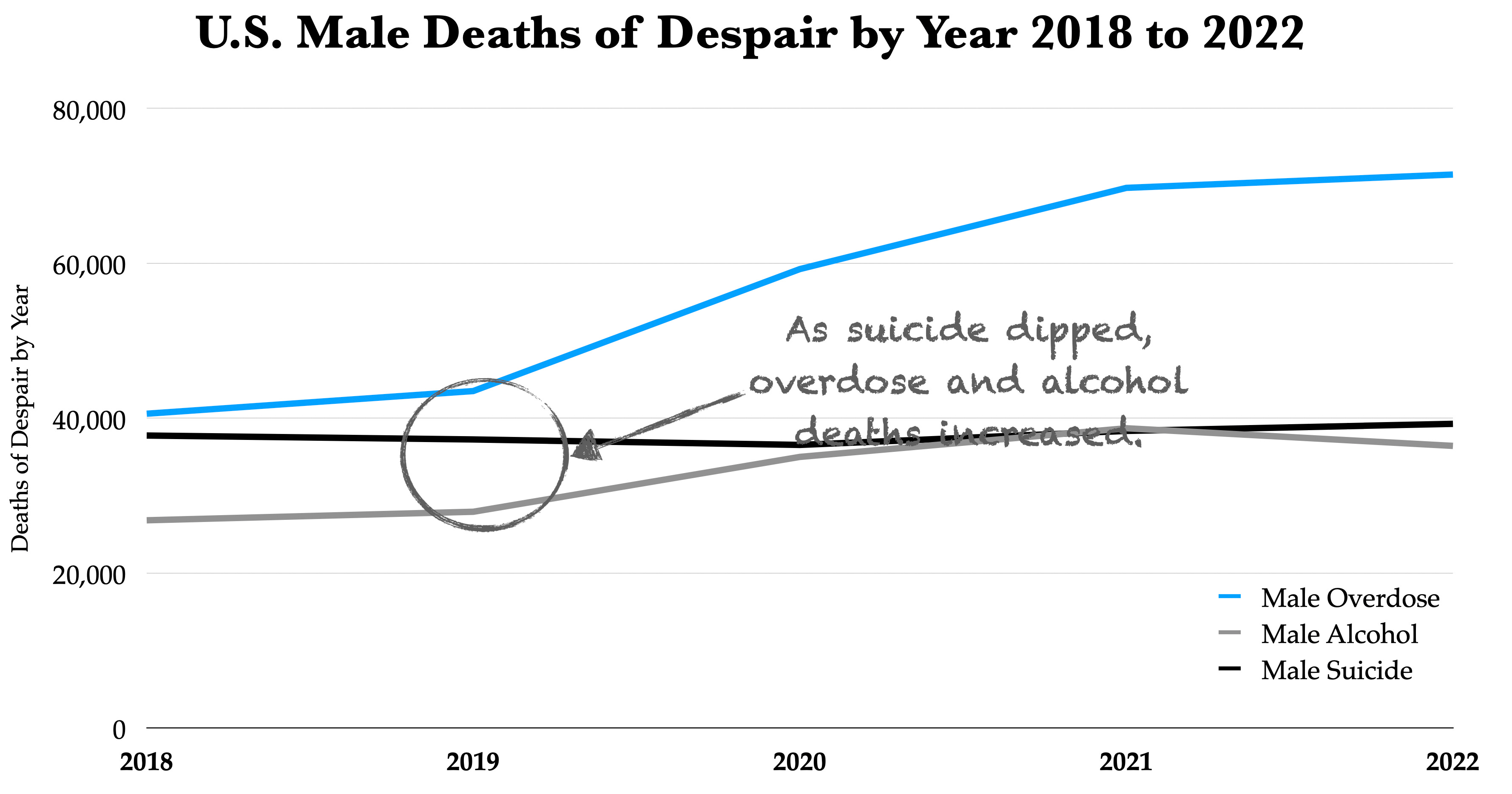
Suicide, overdose, and alcohol abuse are not the despair; they are the response to the despair, the pain, the risk.
There are a host of reasons, such as males are more likely to turn to self-medicating as a way to cope with depression and even physical pain; we saw this with the opioid crisis that started in the early 2000s (KFF). And in California, men have accounted for 77-78% of the opioid deaths from 2020-2022. We are also seeing more young men, especially those without post-secondary degrees, turn to greater marijuana use, other drugs, and alcohol use. While some of this is recreational, there are far too many who use it as a form of self-medicating to mask underlying issues or deal with serious mental health issues.
And with males less likely to find therapists, drop out of therapy, and become therapists themselves who understand the needs of men and who come from a brain-sex difference approach first, it just gets harder. Roughly 77% of mental health counselors are female and 23% are male. It should be noted that some female therapists do work with men and take on an approach that looks at sex differences. But for some men, a male counselor may be needed in the same way some women prefer a female counselor.
While attempts are being made to address suicidal ideation, drug and alcohol addiction, and other challenges, enough is not being done for our boys and men, particularly in states like California that have established a California Commission on the Status of Women and Girls and other agencies designed to specifically look at female outcomes while generally ignoring male outcomes. And while it’s wonderful, for instance, to celebrate a decrease in suicide deaths in any particular year for males or females; it usually means an increase in another area of despair, such as overdose or alcohol, as the graphs above show. This partly happens because we ignore the brain-sex differences that impact the way males and females cope with depression and the support and courage needed to seek therapy with therapists who understand this difference.
Understanding male despair is a pressing need and one we can undertake and one parents and those seeking counseling should take seriously before entering therapy.
Although I’m not a therapist, here are some simple questions you can ask a therapist before beginning therapy for yourself, your son, your daughter, or your family?
Do you believe that males and females handle depression differently? If so, how? If not, why not? (If the therapist relies on social norm theories to express himself/herself, it is probably not the right fit. If the therapist starts talking about the ways males and females process depression in the brain and how their actions and expressions manifest differently, not as rights or wrongs but reactions regulated by processes within the scope of brain-sex difference, you are probably on the right path.)
What do you believe plays a bigger role in mental health, sex or gender? Is there a difference between sex and gender? How would you explain it? (If the therapist overemphasizes gender in a way that blurs it with sex or that suggests sex is not the first principle, I would probably not use that therapist. For me, I would be looking for the therapist that emphasizes sex-difference over gender and does not muddy the waters—seeing sex as the first principle and gender as a social construct that is more elusive.
Phrases to watch out for include “sex-assigned at birth” or “gender assigned at birth” because sex (male/female) is something we all participate in while gender is something more elusive and predicated on constructs. Sex is not assigned. It is certain, and so are many of the processes that impact mental health.
So much of what we see happening to our boys and young men occurs because, honestly, policy makers and so many others are feeling the social pressures entrenched in academia, media, and government that rightly support women and girls and are simultaneously fearful of the backlash of supporting boys and men, are uneducated about the outcomes and reasons and—too—rely on masculine social norm theories instead of brain-sex difference to bypass boys and men altogether, usually for some political advantage or social acceptance.
California, like so many states, could change course and break away from these fears and harmful stereotypes. The first step could be a California Commission on the Status of Boys and Men as a way to start getting at the root causes of so many troubling outcomes that often start because we do not begin with the first principle, xx and xy.
Event Update
Join Global Initiative for Boys and Men for it’s upcoming event in Pleasanton, CA.
Paul, thanks for this informative response and making sure we do not forget the cultural component that dehumanizes the male and does not address male needs and pits males against females. A case in point is the recent announcement by Jill Biden that the Dept. of Defense will be adding 1/2 a billion to women's health. She suggested that research ignores female bodies. This is completely untrue. This cliché remains overused and wrong, and the CDC has already reported there is “no evidence of any systematic under‐representation of women in clinical trials.” Besides, men instinctively want to protect women. It's time for the dialogue to include men too.
Sean, your point about differences between male and female brains is well taken. It took many years for me to understand that, but I do now. And yet I worry that you go too far in stressing the primacy of nature over culture. The relation between them is not that simple.
Though constrained by nature, culture is always, perhaps ironically, a product of nature. Every man is a combination of maleness and masculinity (no matter what the latter's form in any time or place), just as every woman is a combination of femaleness and femininity (no matter what the latter's form in any time or place). By definition, humans are innately--biologically--culture-creating animals. A cultural system, such as gender, does not amount to a superficial veneer. I'm not suggesting that any particular gender system is either healthy or unhealthy, only that gender, like sex, is a reality in every society. We ignore it at our peril.
You won't disagree with that. But that's merely the prologue to what I really want to say here. Boys and men suffer not only from this or that notion of masculinity--whether "traditional" or "progressive"--but also from this or that notion of femininity. This is because boys and men live in the same world as girls and women. In other words, girls and women (especially mothers) always have a say in how culture defines masculinity.
But here's my point. I suggest that one of the central problems for boys and men in our time is the relentless and implacable attack on masculinity and even on maleness by feminists (including those who happen to be male). This is a gender war, not a genetic one (although it could ultimately have genetic effects if enough men and women fail to marry and reproduce society, which is already becoming problematic in every Western country). I say this because the animosity is cultural in origin, not natural.
From this, it follows that personal therapy will not solve the problem of cultural hostility between
men and women (although a competent therapist could, of course, help individual patients cope effectively with that conflict in everyday life). What we need is collective therapy, something that I've called "intersexual dialogue." Unlike debate, dialogue is not about one side winning and the other losing. It's goal is not toleration but something more like sympathy, compassion or intimacy. The goal, in a word, is interdependence. And that is possible only by cultivating a gender system that fosters interdependence.
This supports what you've been arguing so well, Sean, but I want to underline how important it is to avoid the extremes of both "social constructionism" and "biological determinism."